Model Performance
XGBoost emerged as the top performer with strong discrimination and excellent calibration
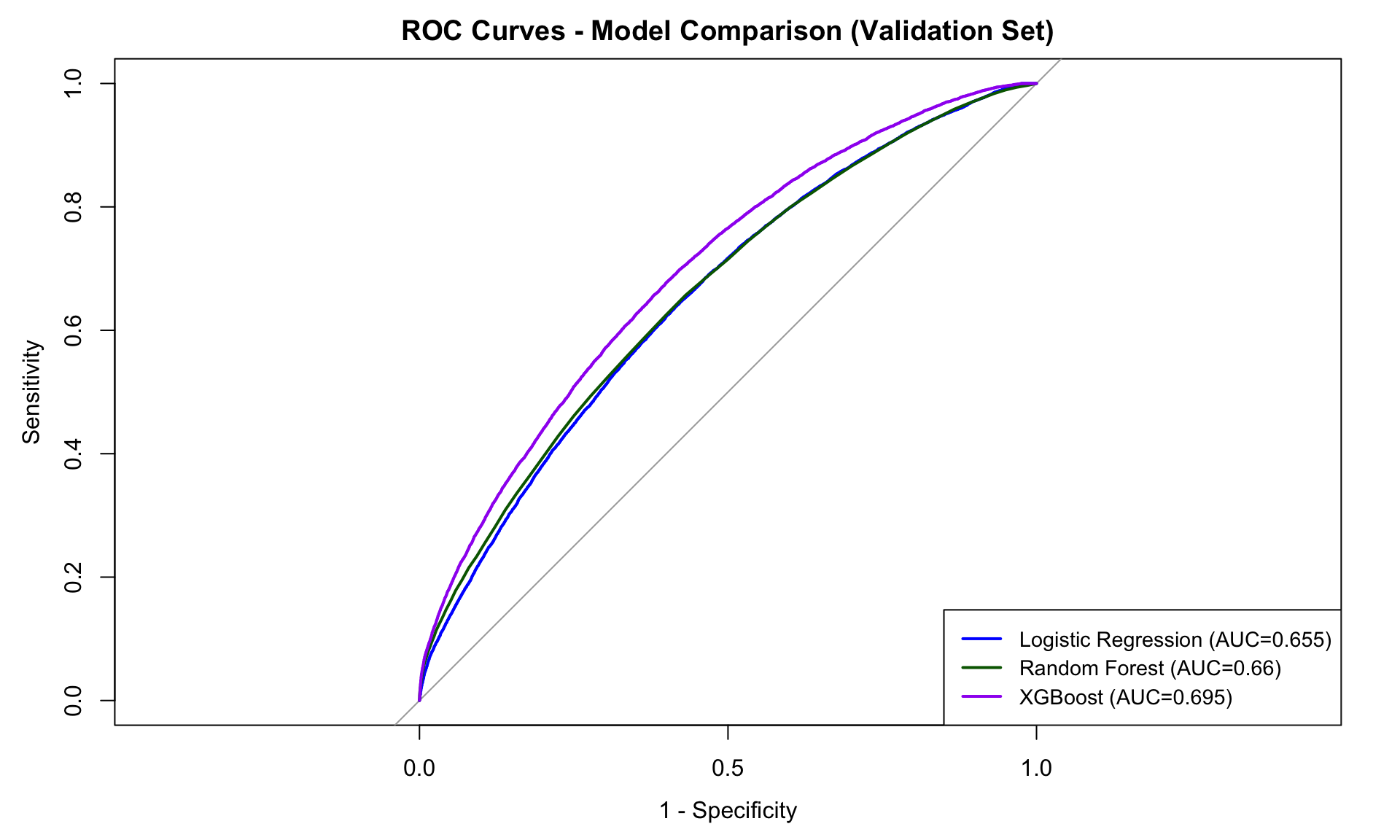
Model Comparison Results
| Model | AUC | Sensitivity | PPV |
|---|---|---|---|
| Logistic Regression | 0.655 | 64.2% | 28.5% |
| Random Forest | 0.660 | 65.1% | 29.2% |
| XGBoost | 0.683 | 68.8% | 29.8% |
Key Finding: The 29.8% PPV represents a 50% relative improvement over the 20% baseline readmission rate, enabling more efficient resource allocation.
Top Predictive Features
Clinical Complexity Score
100%
Charlson Comorbidity Index
87%
Healthcare Utilization
75%
Medication Burden
68%
Length of Stay
54%
Age
42%
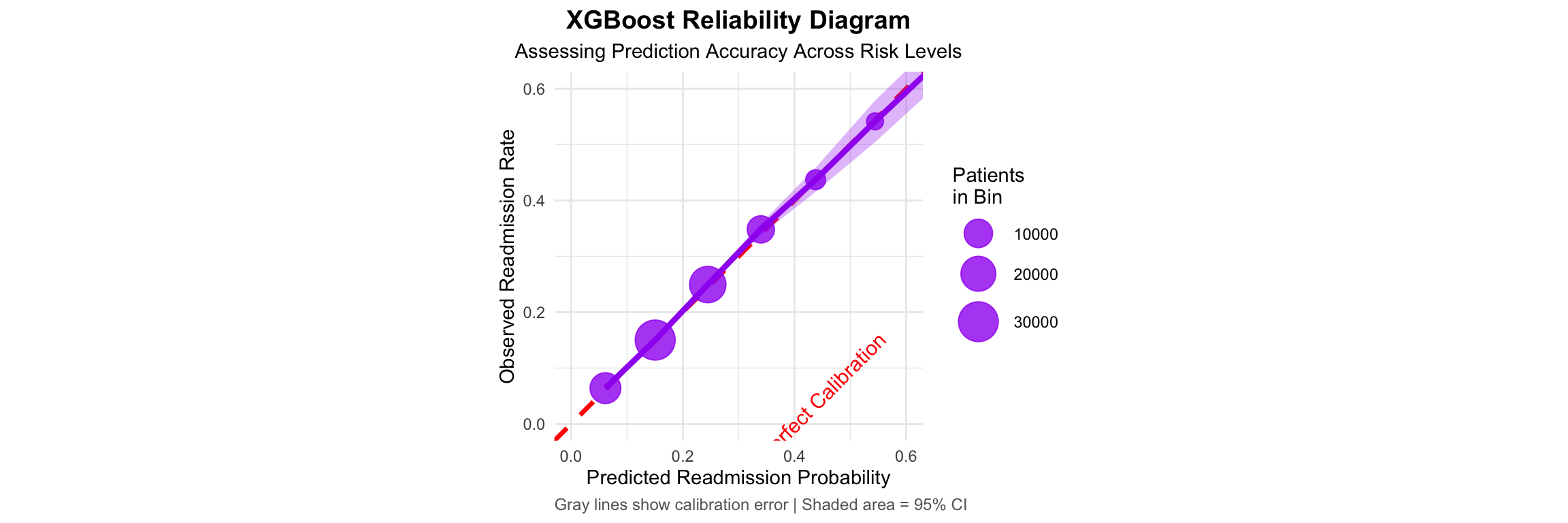
Well-Calibrated Model: ECE = 0.022, indicating trustworthy probability estimates